
Improving Global Sexual and Reproductive Health:
A talk with Dr Rafael Mazín-Reynoso
It all begins with an idea. Maybe you want to launch a business. Maybe you want to turn a hobby into something more. Or maybe you have a creative project to share with the world. Whatever it is, the way you tell your story online can make all the difference. Don’t worry about sounding professional. Sound like you. There are over 1.5 billion websites out there, but your story is what’s going to separate this one from the rest. If you read the words back and don’t hear your own voice in your head, that’s a good sign you still have more work to do.
What do you think are healthy habits when it comes to sexual health?
Sexual health encompasses various areas of the life of people and communities:
To take care of the physical area, it is important to make routine self-exploration to look for any changes, growths, lumps, lesions in genitalia and breasts. Also, to periodically get physical check-ups and vaccinations against STIs such as hepatitis B and HPV.
In the emotional area it is critical to cultivate a pride of one´s gender and sexual identity and live without shame or guilt. Sexuality has to be a source of health and wellness rather than of malaise and discomfort.
In the volitional area one has to develop the capacity to make responsible decisions, free of pressure, coercion or under the influence of a substance or the hazardous, unplanned conditions of certain situations.
In the field of sensual experiences, it is critical to bear in mind that sexuality is the source of pleasure and enjoyment. It is a positive dimension of a healthy sexual life to achieve pleasure from sexual activity. However, it should never result in regrets, shame, or physical or emotional damages to third persons.
In the affective area it is important to behave with honesty, truthfulness, and expression of sincere feelings. Exploitation, falsehoods, and deception are expressions of unhealthy sexuality.
In the dimension of reproduction, it is of paramount importance that it is not desirable to let pregnancy occur by accident. It is a life-time commitment and they have to talk about it to make informed decisions by mutual consent and bear in mind the risks of pregnancy among very young women. A single person may decide to have a child, but it must be clearly understood what it takes to raise a baby. A child is not a toy, a doll. It is a living creature with needs even more complex than those of a pet it is also important to reflect about what the parents-to-be would have to offer to a child in the long term.
Lastly, in the field of social responsibility, it is critical for a healthy sexuality to ask oneself if one´s gender role is flexible and free of toxic stereotypes, if one is ample enough to accept and embrace different sexual orientations, models of family, relationships among people from different origins. Prejudices, phobias, rejection, disdain are expressions of absence of sexual health.

To what extent, if any, is abstinence a good form of sex education?
There have been efforts by some groups and organizations to advance an approach to sex education based on abstinence, known precisely as “as abstinence-only sex education”. This approach is centered on omitting any reference to and provision of information about contraception and sexual activity, including masturbation, before or outside a heterosexual marriage. Thus, it deprives young people of critical information to make responsible, autonomous, and gratifying decisions.
A 2007 federal study on abstinence education in the USA found that these programs had no impacts on the rate of teen sexual abstinence. The US congress has already started taking some action to improve sex education across the country. Part of that process is the personal responsibility education program [PREP -not to be confused with pre-exposure prophylaxis]. With PREP, both abstinence and contraception are supposed to be emphasized. Still, abstinence-only is an incomplete, dismembered form of “education” that robs youth of evidence-based information and of the opportunity to acquire the capacity to make mature decisions.
Why is it important to support the education of young people on sexual and reproductive health?
What is not taught in a systematically planned way, presented in a school setting or taught through extramural activities will be learned in a distorted, incomplete way, full of myths and prejudices in any other spaces. Society has to opt for organized, structured, and systematic processes, not for the conventional learning of distorted, incomplete, mendacious, and prejudiced processes that have been occurring for ages in the street and other spaces not intended for formal education.
Is there any room for improvement regarding promotion of sexual and reproductive health?
Yes, school staff needs to be trained. As any other members of the society they have many knowledge gaps and distorted ideas, myths and prejudices. This also applies to health care staff who have had limited or no training in sexual health during their pre-service training. Last, but not least, it is important to work with community-based organizations to ensure they are facilitators in processes of promotion of sexual and reproductive health. In addition to this, education and health authorities must be persuaded about the necessity of promoting sexual and reproductive health, using for that evidence of the impact on public health indicators.

How would you describe the influence of religious practices on access to sexual and reproductive health services?
Religion, properly understood, should make deeply observant people live their lives according to universal ethical principles that would make them not only very respectful and sympathetic of the needs of third persons, but also deeply fulfilled, very happy. Unfortunately, there are many policy and decision-makers who shield themselves behind “religious principles” to hamper the functioning of sexual and reproductive health services. Last week, a US senator who claims to be ”too deeply religious” stated that “pregnancy does not entail risks to life”. I would say that religion is lived in different ways by people who may assume their religiosity is a key to openness and use of scientific and technological development from others whose religiosity make them perceive the body, health care and science as intrinsically evil.
In sum, I would say that, like in any human field, there are deeply religious people who are educated, smart, and sympathetic. They care about expansion of access to comprehensive care services. On the other side are the fundamentalists, who function with dogmas, irrational beliefs (instead of knowledge), and lack of empathy. These individuals will manifest a violent opposition. Still, it is not religion per se, but the people who have remained in darkness. Public health policy-makers must have the deepest respect for believers and yet must prevent irrational beliefs from interfering with protection and care of the sexuality, reproduction, health and life of human beings.
What is the most effective way of reducing inequality in access to SRH services, especially for vulnerable groups, e.g. those with low socioeconomic status?
Community-based outreach using either the “navigators” model or creating services in the community.
How successful is prevention of STIs in countries with good quality sex education compared to countries where the topic might not be thought at all?
The World Health Organization recommends comprehensive sexuality education along with STI and HIV pre- and post-test counselling as a first pillar in the prevention of STIs. However, it is difficult to establish a reliable comparison because different regions of the world report STI using a syndromic approach, whereas others use an etiological approach. Moreover, the diseases are not required to be notified in all the countries. Also, available data are mostly from key populations. Yet, it can be said that sound sex education is a protective factor.
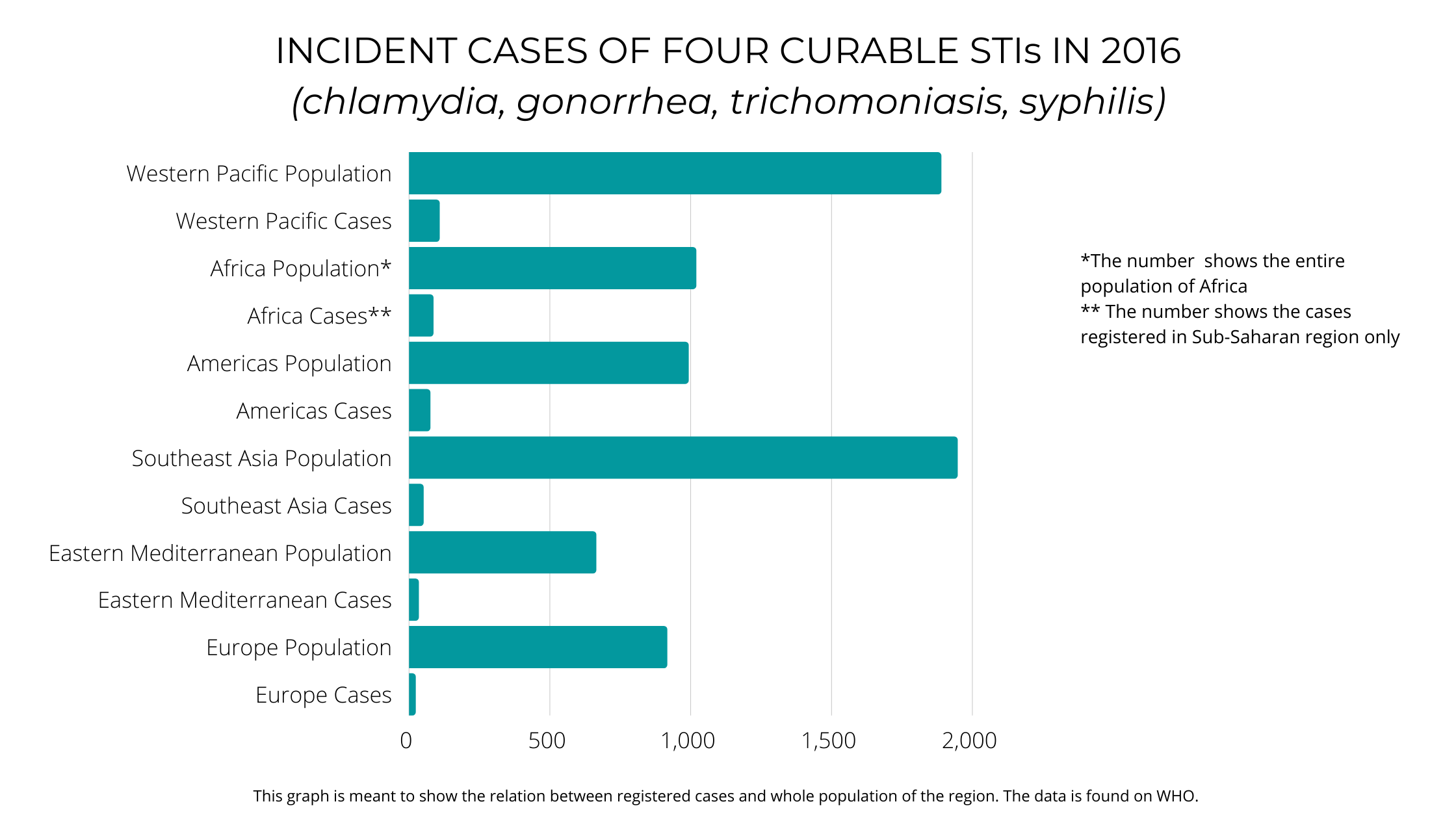
Estimates for 2016 made by the World Health Organization resulted in a number of incident cases of four curable STIs (chlamydia, gonorrhea, trichomoniasis, syphilis) of about 376 million new cases, globally. The largest number was calculated for the Western Pacific Region, that includes China (108 millions) and Sub-Saharan Africa (86 million), followed by the Americas (75 million), and then Southeast Asia (51 million), the Eastern Mediterranean Region (34 million) and Europe (23 million). Even if the information on incidence of STIs is available through estimates, information about school-based sex education is scarce and programs may change with every entering administration.
Russian authorities actively disregard the wellbeing e.g. MSM (men-who-have sex-with-men). How would you describe comprehensive care for homosexuals and transgender people?
Disregard for the health, wellbeing and the life of any group, community or population on any basis is a disgraceful, loathsome, and contemptible. When the disdain, marginalization, and mistreatment come from so-called “healthcare authorities” the only word to describe the behavior of those violators of a universal ethical code that must apply to all care providers is “vile”. It is shameful that in the XXI century we still this type of behavior.
The comprehensive health care for persons who have sex with others of the same sex and transgender people starts and stays grounded in deep respect, compassion, desire to help and to understand the needs and demands of these groups and populations. Once their needs are identified, the responsible, committed, respectful, and qualified provider implements a clinical protocol that might be related to the physical, emotional, volitional, affective, sensual, and reproductive dimensions of their sexual health.

Somalia might approve child marriage, some claim to protect their daughters.
Are they really protected and how does getting married so young affect their sexual health?
No, absolutely no. This practice may encourage intergenerational sex of which there is overwhelming evidence that it puts young girls at risk of contracting HIV and other STIs, including HPV. Additionally, the genital tract of a very young woman is not fully mature and amenable to lesions and lacerations during intercourse. If they get pregnant their pregnancies entail high risk of complications and death.
Perhaps the most worrisome of this dreadful policy is the lack of respect and consideration for the young girl whose right to make informed decisions is completely ignored. It is contemptible that in the XXI century young women are seen as objects, as cattle whose fathers “give in marriage” under to grotesque pretext of “defending” them.
Sex-Ed should include safety and enjoyment.
Yet, enjoyment is rarely included. In what ways does leaving this out affect young people’s sexual health?
Pleasure is critical component of human sexual behavior. It is very likely that the vast majority of episodes of sexual activity occur because people indulge in something that “feels very good”. Ignoring that has made of sex-ed an uninteresting topic.
In fact, promotion of condom use must be associated to strategies to ensure the use of this commodity is pleasurable. Pleasure is a critical element of health and wellbeing.
The Editorial team thanks Dr Rafael Mazín-Reynoso on behalf of CGHI for the kindness and time taken to complete this interview.
This article was written by Ana-Marija Meglic.
As Editorial Officer and emerging public health professional she develops global health content for CGHI. She applies her health education and communication skills to increase public awareness.
